
Have you ever been told you have runner’s knee? Do you suffer from knee pain underneath your kneecap during or after you run? Does it impact how often and how long you can run for?
Runners Iove nothing more than to run; whether that’s alone, with friends, in a club, through the fields, on the road, or in the gym. Anything that prevents this can have a huge impact on a runner’s ability to achieve their goals, maintain their physical fitness, and look after their general well-being.
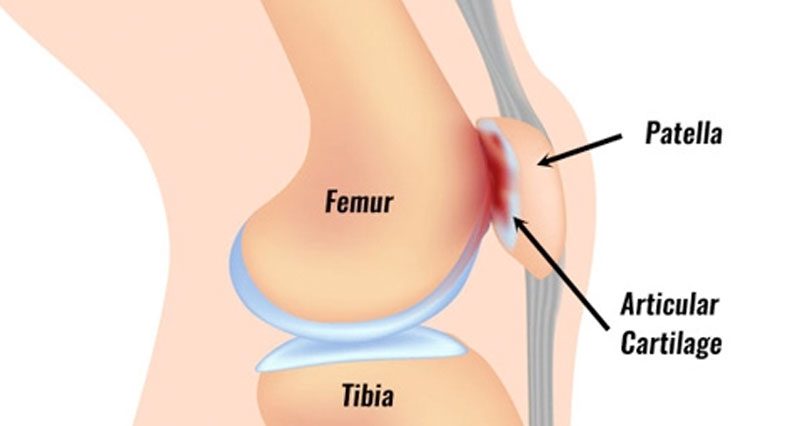
Knee pain during or after running is common and can have a huge impact on an activity that is important for your physical and mental well-being1. A common diagnosis of this pain is patellofemoral pain syndrome (PFPS), this is an umbrella term which can encompass many different structures including the patellofemoral joint (behind the knee cap), iliotibial band, patella tendon (below the knee cap), fat pad or bursa (sac of fluid)1. Finding the exact structural diagnosis can be challenging, however contributing factors and management are often very similar. In the past this condition has often been diagnosed as chondramalacia patella, however this structure has since been found not to produce a pain response2. Therefore, this diagnosis has largely been dismissed as the driver of knee pain.
The tell-tale sign a physio will be searching for is pain behind the kneecap and the base of your femur (thigh bone). This can be tested when compression is put through the kneecap when the leg is straight or when the patient contracts the thigh muscle which reproduces the pain. The pain occurs when the kneecap is overloaded in the patella groove of the femur and is likely due to the patella poorly tracking in this groove which causes friction in this site.
A variety of factors have been investigated, with one study claiming over 500 factors are potentially contributing to PFPS3. Typically, in runners, knee pain can be explained by an increase in mileage, a sudden introduction of speed or hill work, a change in running surface or insufficient recovery between training. Other areas that are often identified that may contribute are quadricep (thigh) and gluteal (buttocks) weakness, reduced movement control, reduced flexibility, or specific running gait patterns1,2,3,4.
These contributing factors are individual to each runner meaning there is no one recipe to success, rather an individualised assessment of training habits, gait, strength and flexibility is often key.
Numerous treatments have been researched and used in the treatment of PFPS however the latest research indicates it is largely down to load management, alongside specific strengthening and possibly gait retraining1, 2. Load management was first proposed by Dr Scott Dye (2005)2 where he highlighted the idea of tissues requiring load for adaptation alongside the risk of overloading tissues leading to pain and dysfunction. This suggests tissues need exercise/load to adapt and strengthen however too much load or too frequent load can cause pain or injury.
There are several ways in which this can be managed and it often requires a tailored programme to your unique needs, abilities and deficits. However, it is worth noting that it is rare that you will need to stop running for this and can still likely achieve your goal but would benefit from assistance in planning your training around this as well as with complementary treatment to manage the pain during this time!
If this is or other aches and pains are affecting your running or other activity Oxon Physiotherapy can help to provide the right guidance to help you achieve your goals.
Crispin Mortimer